
Introduction
Chronic recurrent multifocal osteomyelitis (CRMO) is part of a spectrum of diseases characterised by chronic non-bacterial inflammation of the bone and is classified as an autoinflammatory disease due to its presumed genetic predisposition and the immune mechanisms involved.
Epidemiology
This is a rare disease whose exact incidence is unknown. It occurs more frequently in childhood than in adulthood (at the age of 7–12 years, 2–4 times more often in girls). In younger children, extremely rare genetically determined osteitis (e.g. as part of DIRA syndrome) must also be considered. In adults, it is more often associated with skin manifestations (e.g. SAPHO syndrome – synovitis, acne, pustulosis, hyperostosis, osteitis).
Etiopathogenesis
The exact aetiology is unknown and a genetic component is assumed. The pathogenesis of osteitis probably involves an abnormal response of neutrophil leukocytes and increased production of IL-1β (independent of inflammasome). CRMO is etiopathogenetically similar to other diseases: spondyloarthropathy (it can progress into it), psoriasis, palmoplantar pustulosis and chronic intestinal inflammation.
Clinical picture
The clinical picture has a chronic or, more often, fluctuating course, with activity alternating with remission. There are no validated diagnostic criteria, diagnostic biomarkers, or precise definition of inactive disease/remission. It is a diagnosis per exclusionem based on clinical manifestations, imaging tests, and possibly bone biopsy.
The main clinical manifestations include localised bone pain, sometimes accompanied by swelling of the adjacent soft tissues and fever. Synovitis may be present distally from the affected bone.
Other manifestations include palmoplantar pustulosis in about 25% of cases (see Figure 1), and in adolescents and young adults, severe pustular acne (SAPHO syndrome) may be present.
The most commonly affected bones are the metaphyses of long bones, the clavicle, vertebral bodies and pelvis (see Figure 2). The number of bone lesions varies (sometimes only a single lesion, more often multiple lesions). Sometimes, even asymptomatic lesions are revealed by bone scintigraphy or whole-body magnetic resonance imaging (WB MRI).
Examination
Basic examinations include laboratory tests, imaging methods and bone biopsy.
Laboratory tests may or may not show signs of inflammatory activity (FW, CRP, leukocytosis). There may also be no association with HLA B27.
The basic examination is a native X-ray of symptomatic areas (see Figure 3), supplemented by magnetic resonance imaging and/or computed tomography.
The optimal imaging technique is whole-body magnetic resonance imaging (WB MRI), which reveals asymptomatic lesions and shows extraosseous involvement (myositis, synovitis).
Other examinations include bone scintigraphy, which displays the administered radiopharmaceutical in proportion to the intensity of metabolism and blood supply.
We indicate bone biopsy mainly in monofocal processes or atypical diseases to rule out other (tumour, infectious) aetiologies. The appropriate site is selected based on the findings of imaging methods. Typical findings depend on the duration of the lesion.
Differential diagnosis
The differential diagnosis includes infectious osteomyelitis (bacterial, mycobacterial, fungal), bone tumours and metastases (primary intraosseous lymphoma, osteosarcoma, Ewing’s sarcoma, leukaemia, neuroblastoma), benign bone lesions (osteoid osteoma and osteoblastoma), Langerhans cell histiocytosis, Rosai-Dorfman disease, psoriatic arthritis, spondyloarthropathy and hypophosphatasia.
Treatment
Non-steroidal anti-inflammatory drugs are the first-line treatment. If they are not effective enough, we add corticosteroid therapy (short-term, during exacerbations), bisphosphonates (especially pamidronate, recommended particularly for spinal involvement) and biological treatment (especially TNF-α blockade).
Prognosis
The prognosis is variable; the disease typically progresses with temporary exacerbations and remissions of varying lengths. Spinal involvement is the most serious prognostic factor.
Appendix: images
Image No. 1
Palmoplantar pustulosis in a patient with CRMO

Image No. 2
Comparison of bone lesion distribution on MRI in children with CRMO and septic osteomyelitis (according to Schnabel et al., 2016)
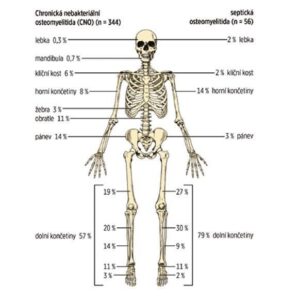
Image No. 3
Enlargement and osteolytic lesions of the medial end of the left clavicle and soft tissue oedema on X-ray

Septic arthritis and osteomyelitis
Introduction
Septic arthritis and osteomyelitis are ACUTE CONDITIONS in paediatric rheumatology due to the risk of septic complications and irreversible damage to the joint or bone. They involve the presence of live bacteria in the joint cavity (septic arthritis) or bone (osteomyelitis). They can occur separately or together. The clinical picture depends on the age of the child and the virulence of the microorganism.
Epidemiology and etiopathogenesis
It most commonly affects young children between the ages of 2 and 5. The overall incidence is 10–20 cases per 100,000 children per year. It most commonly arises from haematogenous spread from another focus (respiratory tract, ENT area, skin infection) and direct transmission (e.g. deep thorn, injury, surgery).
The most common pathogens causing joint and bone infections in children
| Age | Microorganism |
| < 12 months | Staphylococcus aureus Newborns: Group B streptococci, G- rods |
| 1–5 years | Staphylococcus aureus, group A streptococci, pneumococcus, Haemophilus influenzae, Kingella kingae |
| 5–12 years | Staphylococcus aureus, group A streptococci |
| 12–18 years | Staphylococcus aureus, pneumococcus, group A streptococci, Neisseria gonorrhoeae |
| in sickle cell anaemia, immunodeficiencies Salmonella |
Septic arthritis occurs in 50% of cases within two years of age, and in 75% of cases the joints of the lower limbs are affected (knee > hip > ankle) (see Figure 4). Osteomyelitis is most commonly localised in the metaphysis.
Factors for the clinical prediction of septic arthritis (adapted from Kocher et al., 1999) include fever (> 38.5 °C), inability to stand or pain during passive joint movement, FW > 40 mm/h and leukocyte count (> 12 x 109). The more factors that are present, the greater the likelihood of the disease.
Clinical picture – typical symptoms
The typical clinical picture includes acute onset and rapid progression (hours to days) with general symptoms (fever, fatigue).
A comprehensive clinical examination (of the entire musculoskeletal system) is ALWAYS necessary. Usually, one location is affected. In cases of multifocal involvement, immunodeficiency must be considered; in cases of multiple vertebral involvement, tuberculosis and metastases must be suspected.
We consider bone or joint infection in children with sudden onset of fever, unexplained limping and/or abnormal limb posture, refusal to use the limb, limited range of motion, musculoskeletal pain ± localised tenderness of the joint or bone, and swelling with redness (see Figure 4). CAVE: young children cannot localise pain accurately (e.g. pain transferred from the hip to the knee area).
Clinical picture – specific situations
Specific situations include infections in newborns and infants, specific infections, subacute and chronic osteomyelitis, spondylodiscitis and purulent sacroiliitis.
In newborns and infants, any infection generally manifests itself through general symptoms (e.g. temperature instability, heart rate disorders, circulatory disorders, tachypnoea, alteration of general condition, etc.), and local findings may be poor at first (e.g. in hip joint infection, there may only be painful abduction during nappy changing). If we observe joint or bone pain or swelling during a clinical examination in this age group, we must rule out fracture or purulent inflammation. Reactive arthritis is rare in children <1 year of age and is often pyogenic inflammation. Tissue destruction by inflammation is more extensive than in older children, and therefore osteomyelitis and septic arthritis are included in the differential diagnosis of young infants with unknown infections.
Specific causative agents include Mycobacterium tuberculosis or the BCG strain (milder course). The onset of symptoms is gradual and dominated by fatigue, weight loss and night sweats. The spine is most commonly affected (with destruction of spinal cord compression and paraplegia), followed by the sacroiliac joint, hip, knee and ankle. Paravertebral abscesses and their drainage into the pelvis are typical. Examination and treatment at a specialised facility is necessary.
Subacute and chronic osteomyelitis typically occurs when the bacteria are less virulent, the individual’s immune system is stronger, or antibiotics are used. Treatment consists of excochleation under antibiotic cover.
Spondylodiscitis is an acute purulent inflammation of the vertebral and intervertebral discs. Symptoms include fever, fatigue, back pain and often abdominal pain. It is treated with antibiotics, immobilisation and surgery in the case of abscess formation.
Purulent sacroiliitis causes pain in the back, abdomen, hip and thigh. Treatment is the same as for spondylodiscitis.
Examination
Basic examinations include laboratory and imaging methods.
Laboratory tests reveal non-specific inflammatory markers (↑FW, ↑CRP, neutrophilic leukocytosis with shift). It is important to identify the causative agent of the infection BEFORE starting antibiotic treatment.
1. Repeated blood culture (three days in a row)
2. Direct culture from effusion or tissue (CAVE – a negative result does not rule out septic origin – synovial fluid inhibits bacterial growth in media)
3. Detection of bacterial DNA by PCR (so-called panbacterial 16S rRNA)
4. Exudate microscopy: Gram staining (detection rate approx. 70%), cytology (> 50,000 leukocytes/μl with > 90% neutrophils), macroscopically purulent
Imaging methods include native X-ray, joint sonography, computed tomography, magnetic resonance imaging and bone scintigraphy. For both X-ray and sonographic examination of the limbs, the general rule is to image both the affected and contralateral areas for lateral comparison. The indication and interpretation of further imaging is the responsibility of the paediatric orthopaedic surgeon or surgeon.
Differential diagnosis
The differential diagnosis of septic bone or joint processes includes other acute arthritis (parainfectious and postinfectious), Lyme arthritis, chronic recurrent multifocal osteomyelitis, bone tumours, acute leukaemia and the systemic form of JIA.
Treatment
Treatment is complex and multidisciplinary (paediatrician, orthopaedic surgeon, microbiologist/infectious disease specialist, and possibly a physiotherapist and prosthetist). Initially, hospitalisation in a surgical or orthopaedic facility is necessary.
Antibiotics are administered immediately after samples are taken for culture, without waiting for the results. Treatment is started empirically, taking into account the patient’s age and other background information, always targeting staphylococcal infection primarily. Treatment always begins intravenously (for at least one week), followed by a switch to oral administration after a decrease in CRP, normalisation of blood count and signs of improving clinical symptoms (fever, pain, limited mobility).
The duration of treatment is individual, usually three to four weeks for septic arthritis and longer for osteomyelitis.
The regimen is rest with immobilisation of the affected joint. Gentle mobilisation follows once the acute infection has been controlled. Return to full activity depends on the severity of the condition and usually takes weeks to months.
Complications and prognosis
Depending on its duration and the virulence of the microbes, septic inflammation can lead to damage to the cartilage and bone with a number of permanent consequences, including destruction of the growth plate and stunted growth of the limb. The prognosis is worse for hip involvement and in newborns. The prognosis depends on early and adequate treatment.
Appendix: images
Image No. 4
Clinical findings in septic arthritis

Malignancies
Introduction
Up to two-thirds of children with malignant disease initially present with musculoskeletal complaints such as myalgia, arthralgia, arthritis or bone pain. Systemic malignancies may present with arthritis and lead to a misdiagnosis of JIA. Treatment with glucocorticoids or immunosuppressants may delay the correct diagnosis and thus worsen the overall prognosis, induce the development of tumour lysis syndrome or worsen the response to chemotherapy. To confirm the diagnosis and treatment, it is always necessary to refer the patient to a specialised paediatric haematology-oncology centre as soon as possible.
The most common systemic malignancies with musculoskeletal manifestations include leukaemia, lymphomas and neuroblastoma. Tumours of the bones and joints mainly have local manifestations.
Leukaemia
Accounts for 30% of all malignant diseases in children, with acute lymphoblastic leukaemia (ALL) predominating, peaking in incidence in infancy (similar to JIA).
Musculoskeletal manifestations are usually accompanied by non-specific constitutional symptoms such as elevated temperature or fever, fatigue, loss of appetite and weight loss. Intense continuous pain, often localised in the metaphysis of long bones, is typical and may also be present at night. If joint pain is present, its severity usually significantly exceeds the objective findings of arthritis intensity, and morning stiffness is not usually present.
Examination and diagnosis:
The diagnosis involves a combination of clinical evaluation, laboratory tests, imaging methods, and bone marrow aspiration.
Laboratory tests focus on blood counts and biochemical tests.
- Blood count: progressive (usually normocytic) anaemia, sometimes with a decrease in thrombocytes and leukocytes
- Blood smear: may not show leukaemic cells at the onset of ALL (so-called pre-leukaemic phase) and for several weeks (up to months) after the onset of musculoskeletal symptoms.
- Biochemical tests: increased cell turnover markers (LD, uric acid) and non-specific inflammatory activity (FW, CRP)
The sensitivity and specificity of the combination of abnormal blood count and night pain for ALL is 85%.
Plain X-rays of long bones may show streaks in the metaphysis, periosteal reactions, or sclerotic and osteolytic lesions.
The diagnosis is confirmed by a paediatric haematologist-oncologist based on bone marrow examination.
Treatment
During the differential diagnosis process, symptomatic treatment with analgesics or non-steroidal anti-inflammatory drugs is recommended. CAVE: do not administer glucocorticoids. If ALL is suspected, the patient should be referred to a specialised paediatric haematology-oncology centre as soon as possible. Once adequate treatment for ALL has been initiated, the symptoms of arthritis usually disappear.
Lymphomas
This is the most common generalised malignancy in adolescents. Musculoskeletal (MSK) manifestations are less common than in ALL. Bone pain may be present (lymphoma invasion of the cortex and marrow, hypertrophic osteoarthropathy leading to acute painful periostitis), but arthritis is less common. In the differential diagnosis of lymphoma, it is necessary to rule out systemic JIA, rare bone lymphomas and chronic osteomyelitis. Diagnosis requires imaging of the chest/mediastinum (X-ray/CT), abdomen (ultrasound/CT) and histological examination of the lymph nodes (preferably excision of the entire lymph node rather than biopsy).
Neuroblastoma
Neuroblastoma is the most common solid malignant tumour in toddlers with early generalisation. It is a tumour in the adrenal medulla or paravertebral sympathetic ganglia. 75% of children have metastases at the time of diagnosis, and the most common MSK manifestations are bone pain. Warning signs include back pain in young children/toddlers.
Examinations for suspected neuroblastoma include imaging of the abdomen and mediastinum (sonography, X-ray, CT, MRI), X-ray of the bones, bone scintigraphy and laboratory tests (increased FW, neuron-specific enolase, ferritin, LD, increased excretion of catecholamine metabolites in the urine – especially vanillylmandelic acid and homovanillic acid).
Primary tumours of bones and joints
Bone tumours (both malignant and benign) can manifest as pain and swelling. Malignant tumours are rare in children but life-threatening. Early diagnosis is essential. Patients with suspected bone lesions should be referred immediately to a specialised paediatric oncology centre.
Warning signs of malignant tumours include pain that worsens at night, swelling (initially of soft tissues, later palpable bone resistance), accidental/pathological fractures at the site of the lesion (5–10%), weight loss, cachexia, and pulmonary metastases – shortness of breath, chest pain, and haemoptysis.
Laboratory tests may show elevated inflammatory parameters, ALP, LD. A plain X-ray will reveal most bone tumours. However, a normal X-ray finding does not rule out a bone tumour. Sonography screens for soft tissue expansion and diagnoses benign lipomas, vascular malformations, etc. MRI, CT, PET-CT, and PET-MRI define the extent of involvement, soft tissue involvement, staging, and detection of metastases, most commonly in the lungs, less commonly in the lymph nodes. Biopsy is an important source of histological classification and grading of the tumour. Staging depends on the histological grade, extent, presence and extent of metastases, and determines further treatment and prognosis (CAVE: evaluation by an experienced pathologist, or review of the findings by an independent “second reader”).
Malignant tumours
In children, the most common types are osteosarcoma (55%, see Figure 5) and Ewing’s sarcoma (35%, see Figure 6), while chondrosarcoma is extremely rare. This group also includes soft tissue sarcomas (rhabdomyosarcoma and non-rhabdomyosarcomas), mesenchymal cell tumours, extraskeletal Ewing’s sarcoma, synovial sarcoma, fibrosarcoma and embryonic sarcoma.
Benign tumours
These occur more frequently in children than malignant tumours, e.g. bone tumours (osteoid osteoma, osteoblastoma, eosinophilic granuloma), connective tissue tumours (fibrous dysplasia, non-ossifying fibroma (see Figure 7)), bone cysts, cartilage tumours (osteochondroma, enchondroma, chondroblastoma) and others (synovial haemangioma and pigmented villonodular synovitis).
Appendix: images
Figure 5
Osteosarcoma of the distal femur

Figure 6
Ewing’s sarcoma affecting the pelvic skeleton

Image No. 7
Non-ossifying bone fibroma

Text prepared by Natálie Sladká Švestková (natalie.sladka@vfn.cz), mainly based on Paediatric Rheumatology in Practice, chapter 10 Acute Arthritis (Andrej Záhornadský: andrej.zahornadsky@nempk.cz) chapter 12 Musculoskeletal Manifestations of Non-Rheumatic Diseases (Hana Malcová: hana.malcova@fnmotol.cz) and chapter 23 Autoinflammatory Diseases (Kateřina Bouchalová: katerina.bouchalova@fnol.cz)
Illustrations number 1,2,3,5,6 and 7 used with permission from Paediatric Rheumatology in Practice, chapter 10 Acute Arthritis (Andrej Záhornadský: andrej.zahornadsky@nempk.cz chapter 12 Musculoskeletal Manifestations of Non-Rheumatic Diseases (Hana Malcová: hana.malcova@fnmotol.cz) and chapter 23 Autoinflammatory Diseases (Kateřina Bouchalová: katerina.bouchalova@fnol.cz).
Illustration number 4 used from https://casereports.bmj.com/content/casereports/2016/bcr-2016-215904/F1.large.jpg
DOLEŽALOVÁ, Pavla and DALLOS, Tomáš. Paediatric rheumatology in practice. Postgraduate Medicine Series. Prague: Mladá fronta, 2019. ISBN 978-80-204-5540-6
More posts for medical professionals




