
Definition
- Expectoration of blood from the lower respiratory tract
- Rare but serious symptom in paediatric patients
- May range from mild, self-limiting episodes to life-threatening pulmonary haemorrhage requiring urgent intervention.
- Far less common than in adults
- often an indication of a serious underlying disorder, including infections, congenital anomalies, vascular malformations, or autoimmune diseases
Haemoptysis in paediatric rheumatology
Acute vs. Chronic Haemoptysis
Acute Haemoptysis
- Sudden onset, usually lasting hours to days
- Often associated with acute inflammation or a sudden exacerbation of an underlying disease
- More likely to be severe and rapidly progressive in children, particularly in pulmonary-renal syndromes
- Causes:
- Diffuse Alveolar Hemorrhage (DAH): A severe manifestation of systemic lupus erythematosus (SLE), ANCA-associated vasculitis (AAV) and Goodpasture syndrome (GPS)
- IgA Vasculitis (formerly Henoch Schönlein purpura): Extremely rare cause of pulmonary haemorrhage but can be associated with severe renal involvement
- Acute flares of ANCA-associated vasculitis (AAV) or lupus pneumonitis.
Chronic Haemoptysis
- Persistent or recurrent blood-streaked sputum over weeks to months
- More likely due to chronic inflammatory lung disease, recurrent alveolar haemorrhage, or a genetic disorder
- Paediatric patients may not always report mild haemoptysis, delaying diagnosis
- Causes:
- COPA Syndrome: A monogenic autoimmune disorder presenting with recurrent alveolar haemorrhage and interstitial lung disease in children.
- Idiopathic Pulmonary Hemosiderosis (IPH): A chronic cause of recurrent alveolar bleeding, leading to iron deposition, anaemia, and pulmonary fibrosis
- Recurrent vasculitis-associated alveolar haemorrhage, particularly in relapsing AAV.
Idiopathic Pulmonary Hemosiderosis (IPH)
- A rare paediatric disorder characterized by recurrent diffuse alveolar haemorrhage
- Aetiology remains unknown, but some cases are associated with autoimmune processes
- Clinical triad: Recurrent haemoptysis, iron deficiency anaemia, diffuse pulmonary infiltrates
- Diagnosis:
- High-resolution CT (HRCT): Shows diffuse ground-glass opacities and hemosiderin deposition
- Bronchoalveolar lavage (BAL): Presence of hemosiderin-laden macrophages
- Lung biopsy: Helpful in atypical cases
- Treatment:
- First-line: Corticosteroids to reduce inflammation
- Immunosuppressants: Rituximab or azathioprine in refractory cases
- Supportive care
COPA Syndrome
- A monogenic autoimmune disorder caused by mutations in the COPA gene (autosomal dominant)
- Clinical presentation: recurrent alveolar haemorrhage, interstitial lung disease, arthritis, and kidney involvement
- Paediatric onset common, with symptoms appearing as early as infancy
- Diagnosis:
- Genetic testing for COPA mutations.
- HRCT: Shows interstitial lung disease and ground-glass opacities
- BAL: Hemosiderin-laden macrophages
- Treatment:
- First-line: Corticosteroids to reduce inflammation
- Immunosuppressants (rituximab, cyclophosphamide)
- Biologic agents targeting IL-6 or TNF-α
IgA Vasculitis (see separate chapter)
- Most common paediatric vasculitis but rarely causes pulmonary hemorrhage
Systemic Lupus Erythematosus and diffuse alveolar hemorrhage (see separate chapter)
- Paediatric SLE often presents with more severe organ involvement than adult-onset SLE.
- Diffuse alveolar haemorrhage (DAH) is rare but life-threatening.
- Risk factors:
- High disease activity (SLEDAI score).
- Lupus nephritis.
- Presence of antiphospholipid antibodies.
- Diagnosis of SLE:
- ANA (≥1:80 titer) – required
- Clinical criteria (Constitutional, hematologic, neuropsychiatric, mucocutaneous, serosal, musculoskeletal, renal)
- Immunologic criteria
- Diagnosis of DAH:
- HRCT: Diffuse ground-glass opacities and alveolar consolidation.
- BAL: Hemorrhagic fluid with hemosiderin-laden macrophages
- Treatment:
- High-dose corticosteroids
- Cyclophosphamide or rituximab
- Plasmapheresis in severe cases
ANCA-Associated Vasculitis in Children (see separate chapter)
- Includes granulomatosis with polyangiitis (GPA), microscopic polyangiitis (MPA), and eosinophilic granulomatosis with polyangiitis (EGPA)
- Paediatric AAV is aggressive, often presenting with rapidly progressive glomerulonephritis (RPGN) and alveolar hemorrhage
- Diagnosis:
- ANCA serology (PR3/MPO antibodies).
- Renal biopsy: Shows pauci-immune necrotizing glomerulonephritis
- Lung biopsy if needed
- Treatment:
- Induction therapy: Corticosteroids + cyclophosphamide or rituximab.
- Maintenance: Azathioprine, mycophenolate mofetil (MMF), or rituximab
- Plasmapheresis in severe cases
Goodpasture Syndrome (GPS) in Children
- Extremely rare in paediatrics.
- Caused by anti-glomerular basement membrane (GBM) antibodies, leading to alveolar haemorrhage and rapidly progressive glomerulonephritis
- Diagnosis:
- Anti-GBM antibody testing.
- Renal biopsy
- Treatment:
- Plasmapheresis
- Corticosteroids + cyclophosphamide.
Conclusion
- Paediatric haemoptysis due to autoimmune diseases is rare but life-threatening
- More common causes of haemoptysis have to be ruled out
- Pulmonary-renal syndromes (AAV, GPS, COPA, SLE) should be promptly recognized and treated aggressively
- Early diagnosis and immunosuppressive therapy are crucial to improving outcomes.
- Future directions include targeted biologic therapies and genetic screening for monogenic causes like COPA syndrome
Differential diagnosis of haemoptysis in children:
- Infectious causes
- Bacterial pneumonia (e.g., Staphylococcus aureus, Streptococcus pneumoniae, Klebsiella)
- Tuberculosis (TB) – Primary or reactivation TB
- Fungal infections (e.g., Aspergillosis, Histoplasmosis, Mucormycosis)
- Viral pneumonia (e.g., Influenza, RSV, Adenovirus)
- Parasitic infections (e.g., Hydatid disease, Paragonimiasis in endemic areas)
- Autoimmune & vasculitic causes
- Primary systemic vasculitis
- ANCA-Associated Vasculitis (Granulomatosis with polyangiitis, Microscopic polyangiitis)
- IgA Vasculitis – Rare pulmonary involvement
- Systemic Lupus Erythematosus (SLE) – Diffuse alveolar hemorrhage, lupus pneumonitis
- Goodpasture Syndrome (Anti-GBM Disease) – Pulmonary hemorrhage and glomerulonephritis
- Idiopathic pulmonary hemosiderosis (IPH) – Recurrent alveolar hemorrhage without systemic disease
- COPA Syndrome – Monogenic disorder with alveolar hemorrhage, arthritis, and renal disease
- Primary systemic vasculitis
- Cardiovascular causes
- Congenital heart disease, pulmonary arteriovenous malformations (AVMs) – hereditary hemorrhagic telangiectasia (HHT), pulmonary hypertension
- Airway & structural abnormalities
- Foreign body aspiration, bronchiectasis, tracheobronchial malformations, neoplasm (rare)
- Trauma & iatrogenic causes
- Hematologic & coagulation disorders
- Thrombocytopenia, haemophilia, coagulopathy (e.g. disseminated intravascular coagulation syndromes)
- Environmental & toxic causes
Diffuse alveolar haemorrhage due to vasculitis
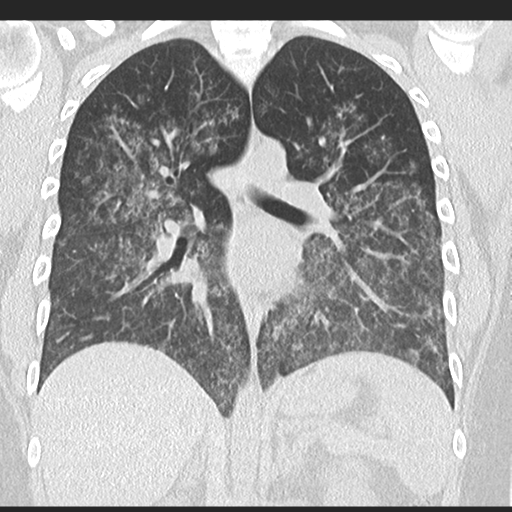
Source: radiopaedia.org
Text prepared by Nikol Husáková (nikol.husakova@vfn.cz), based on following resources:
- Laya BF, Concepcion NF. Hemoptysis in children: Imaging evaluation. Pediatr Radiol. 2007;37(12):1211–1223. doi:10.1007/s00247-007-0609-6
- Weiss PF. Pediatric vasculitis. Pediatr Clin North Am. 2012;59(2):407–423. doi:10.1016/j.pcl.2012.03.005
- Kitching AR, Anders HJ, Basu N, Brouwer E, Gordon J, Jayne DR, et al. ANCA-associated vasculitis. Nat Rev Dis Primers. 2020;6(1):71. doi:10.1038/s41572-020-0204-y
- Tanaka C, Benseler SM. Systemic lupus erythematosus in children and adolescents. Pediatr Clin North Am. 2017;64(2):339–361. doi:10.1016/j.pcl.2016.11.008
- Green RJ, Ruoss SJ, Kraft SA, Berry GJ, Raffin TA. Idiopathic pulmonary hemosiderosis in children: Diagnostic criteria, management, and outcome. Eur Respir J. 2001;17(3):496–501. doi:10.1183/09031936.01.17304960
- Griese M, Kabra SK, Tan HL. Pulmonary hemorrhage in children: Diagnostic workup and therapeutic approaches. Paediatr Respir Rev. 2011;12(3):231–238. doi:10.1016/j.prrv.2011.03.005
More posts for medical professionals

2026-04-16 - 11:51
Lazăr Călin -University of Medicine and Pharmacy „Iuliu Hațieganu” Cluj-Napoca Condition Anamnesis + Physical Examination Labora...

2026-04-15 - 15:49
Lazăr Călin -University of Medicine and Pharmacy „Iuliu Hațieganu” Cluj-Napoca Condition Anamnesis + Physical Examination Labora...

2026-04-14 - 15:33
Introduction Chronic recurrent multifocal osteomyelitis (CRMO) is part of a spectrum of diseases characterised by chronic non-bacterial...

