
Musculoskeletal pain is a common symptom in pediatric practice. It is estimated that in one in 6–10 visits to the pediatric clinic, musculoskeletal pain will be one of the complaints.
Arthralgia is a subjective experience of pain in the joint, while arthritis is an inflammation of the joints indicated by the presence of swelling, tenderness, warmth or redness, and motion pain, with joint stiffness and reduced range of motion commonly observed.
Joint pain (arthralgia) is a common complaint in pediatric outpatient settings. Distinguishing between inflammatory and non-inflammatory etiologies is critical for appropriate diagnosis and management. While many cases result from benign causes such as transient synovitis or hypermobility, joint pain in children may also signal systemic inflammatory diseases or malignancies. This overview provides first-line guidance for non-rheumatology providers on the clinical evaluation, differential diagnosis, and initial workup of joint pain in children.
The most common cause of joint pain among children of all age groups is trauma. However, many benign as well as serious conditions can manifest with painful or swollen joints, including infections, tumors, and systemic diseases. Patient’s history and physical examination play an important role in establishing a diagnosis and determining the extent of further investigations.
In patient’s history, attention should be paid to the age (Table 1) and gender of the child because the frequency of certain causes varies largely depending on these factors (e.g., we will not expect pain due to growth in an adolescent, and/or overexertion syndrome in an infant or a small child).
Table 1. Differential diagnosis of joint pain in children of different ages
| Infant (aged 1–3 years) | Child (aged 4–0 years) | Adolescents |
| transient synovitis | transient synovitis | slippage of the epiphysis of the femoral head |
| fracture | juvenile idiopathic arthritis | overexertion syndromes |
| abuse | Perthes disease | osteochondritis dissecans |
| developmental hip dysplasia | rheumatic fever | |
| juvenile idiopathic arthritis | hemophilia | |
| neuromuscular disease | IgA vasculitis | |
| hemophilia | ||
| IgA vasculitis | ||
| Common causes in all age groups:• trauma (fracture, hemarthrosis, soft tissues)• infection (septic arthritis, osteomyelitis, discitis)• as a part of various viral diseases• tumor• sickle cell anemia• serum sickness | ||
We should find out if the pain appeared suddenly, which is common with trauma or infection, or gradually, which is more indicative of a chronic process. Previous episodes of joint pain are also more indicative of a chronic process than trauma or infection. Furthermore, we should determine if the onset of pain was preceded by trauma (although data on trauma do not exclude a non-traumatic etiology of pain), infection (sore throat, intestinal infection), which may indicate reactive arthritis, or vaccination, which may indicate serum sickness. Information on recent travels, tick bites, and contact with infections should also be checked. We should inquire about the temporal pattern of pain and its duration. Pain that worsens with activity, increases towards the end of the day, and decreases with rest indicates a mechanical disorder, while pain that is most pronounced in the morning and ameliorates with activity, e.g., stretching, points to an inflammatory disorder. Pain lasting a few minutes or hours and resolving spontaneously speaks more in favor of a benign disorder, as opposed to long-term, persistent pain. The patient should be asked about the presence of joint stiffness: information about morning stiffness lasting longer than 15 minutes is particularly important. Pain present at night, refractory to the use of analgesics, and persisting until morning should raise suspicion of a serious underlying condition.
Clinical Approach to Joint Pain
A structured assessment, including history, physical examination, and targeted laboratory and imaging studies, can help differentiate between inflammatory and non-inflammatory joint pain. Key questions to consider include:
– Is the pain inflammatory or non-inflammatory?
– Is the pain acute or chronic?
– Is the pain localized to one joint or multiple joints?
– Are there associated systemic symptoms (e.g., fever, weight loss, fatigue, rash)?
– Are there red flags suggestive of malignancy?
A) Inflammatory Joint Pain
Inflammatory joint pain is characterized by:
– Morning stiffness lasting >30-60 minutes
– Pain that improves with activity
– Warmth, swelling, and erythema of affected joints
– Presence of systemic symptoms (e.g., fever, weight loss, rash)
Common Causes:
1. Autoimmune/Inflammatory Conditions
– Juvenile Idiopathic Arthritis (JIA): Most common chronic inflammatory arthritis in children; can present as oligoarthritis, polyarthritis, or systemic JIA with fever and rash.
– Childhood-onset Systemic Lupus Erythematosus (SLE): Polyarthritis with systemic features such as rash, renal involvement, and cytopenias; positive ANA.
– Juvenile Dermatomyositis: Arthritis with characteristic heliotrope rash and Gottron’s papules, proximal muscle weakness.
– Vasculitides (e.g., IgA vasculitis, Kawasaki Disease): Joint involvement with systemic symptoms such as purpura or prolonged fever.
2. Infectious Arthritis
– Septic arthritis: Acute monoarthritis with fever, joint effusion, and elevated inflammatory markers; requires urgent joint aspiration.
– Lyme arthritis: Mono- or oligoarthritis with a history of tick exposure, often affecting the knee.
– Post-viral arthritis: Self-limited arthritis following viral infections such as parvovirus B19.
3. Reactive Arthritis
– Occurs after a gastrointestinal or genitourinary infection, typically affecting the lower extremities and resolving within weeks to months.
4. Transient Synovitis:
– Most common cause of acute hip pain in children aged 3-8 years
– Typically follows a viral infection and resolves within 1-2 weeks
– Mildly limited range of motion without systemic symptoms
B) Non-Inflammatory Joint Pain
Non-inflammatory pain is characterized by:
– Morning stiffness <30 minutes
– Pain that worsens with activity and improves with rest
– Absence of systemic symptoms
– Minimal or no swelling
Common Causes:
1. Benign Nocturnal Limb Pains (Growing Pains):
– Common in children aged 3-12 years
– Bilateral lower extremity pain, typically at night, resolving by morning
– No associated swelling or systemic symptoms
2. Hypermobility Syndrome:
– Joint pain without inflammation in highly flexible children
– Positive Beighton score indicating joint hypermobility
3. Mechanical/Traumatic Causes:
– Ligamentous injuries, fractures, and overuse syndromes
– History of trauma or repetitive strain
C) Cancer-Related Joint Pain
Joint pain associated with malignancy may arise from direct tumor invasion, paraneoplastic syndromes, or metastatic disease. Red flags include:
– Persistent pain unresponsive to conservative treatment
– Night pain or pain at rest
– Constitutional symptoms (weight loss, fever, night sweats, pallor, easy bruising)
– History of bone pain, back pain, or limping
Common Malignancies:
1. Leukemia: Can present with bone pain, limp, and systemic signs such as pallor, bruising, and hepatosplenomegaly.
2. Neuroblastoma: May cause bone pain and paraneoplastic syndromes with irritability and hypertension.
3. Osteosarcoma and Ewing Sarcoma: Localized bone pain, often at the metaphyses of long bones; may show lytic or periosteal reactions on imaging.
Musculoskeletal Examination in Children
A structured musculoskeletal examination is key to identifying joint pathology (Figures 1-10). The pGALS (pediatric Gait, Arms, Legs, and Spine) assessment, developed by pediatric rheumatologists, is a quick and validated screening tool.
pGALS Screening Questions:
1. Do you (or your child) have any pain or stiffness in your muscles, joints, or back?
2. Can you (or your child) dress yourself completely without any difficulty?
3. Can you (or your child) walk up and down stairs without any difficulty?
pGALS Physical Examination:
– Gait: Observe walking for symmetry, smoothness, and limping.
– Arms: Assess shoulder abduction, elbow extension, wrist and finger movements, and grip strength.
– Legs: Evaluate hip and knee flexion, internal rotation, and ankle dorsiflexion.
– Spine: Inspect alignment and perform forward flexion for scoliosis assessment.
During the clinical examination, which includes inspection, palpation, and examination of active and passive mobility in the joints, attention should be paid to the presence of joint swelling, sensitivity to palpation, skin lesions (psoriasis, systemic lupus erythematosus), systemic signs (fever, diarrhea, weight loss, general weakness, growth retardation), and muscle weakness. All these signs can be associated with serious diseases that manifest with joint pain.

Figure 1 Examination of interphalangeal and metacarpophalangeal joints.
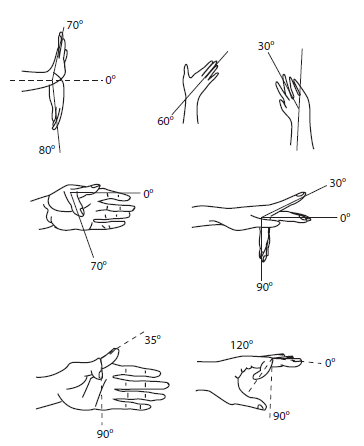
Figure 2 Expected range of motion in individual hand joints (radiocarpal, metacarpophalangeal and interphalangeal).
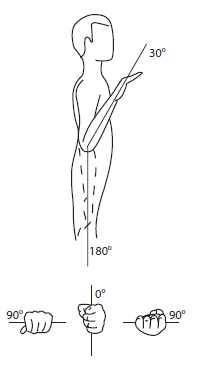
Figure 3 Expected range of motion at the elbow and normal range of motion during pronation and supination.
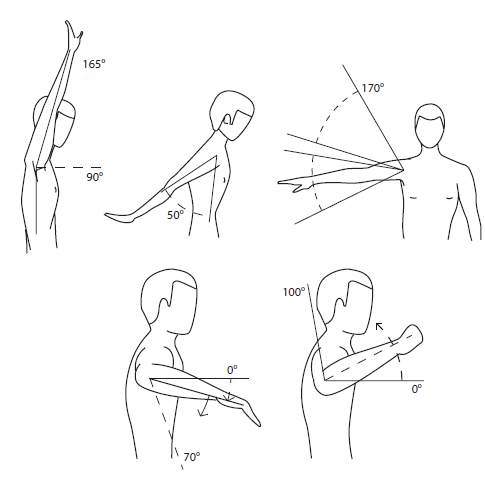
Figure 4 Expected range of motion in the shoulder.

Figure 5 Three-finger test.

Figure 6 Testing of flexion in the thoracolumbar spine.
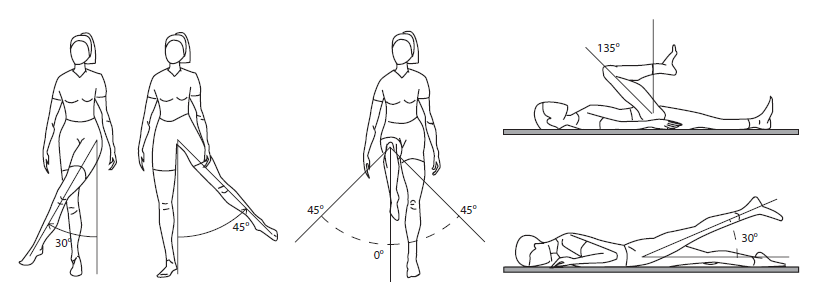
Figure 7 Expected range of motion in the hip joint.

Figure 8 Expected range of motion in the knee joint.
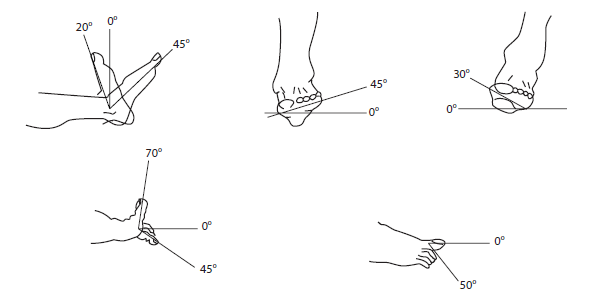
Figure 9 Expected range of motion in the foot, subtalar joint, and metatarsophalangeal, interphalangeal foot joints.

Figure 10 The sites most commonly affected by enthesitis, or the sites of enthesal palpation.
Initial Workup and Referral Considerations
Further diagnostic workup depends on the working diagnosis. If trauma is suspected, imaging should be performed (first of all, X-ray and, if necessary, CT). If an infection or systemic disease is suspected, laboratory workup should be carried out, initially including at least a complete blood count, C-reactive protein, erythrocyte sedimentation rate (ESR), urinalysis, and a bacterial culture of a throat smear. When arthritis is prolonged, tests for rheumatoid factor (RF), anti-CCP, antinuclear antibodies and serum immunoglobulins should be included. Depending on the working diagnosis, the workup can be expanded to include peripheral blood smear, LDH and complete biochemical tests. If osteomyelitis or septic arthritis is suspected, blood cultures should be taken, and if possible, joint fluid aspirate should be obtained for microbiological and cytological analyses. Still, laboratory findings can be normal even in the presence of an infection, tumor or systemic inflammatory disease (especially at the beginning of the disease). Therefore, one should not rely only on the results but take into account the patient’s history and clinical status and closely monitor the patient.
Low Back Pain
Low back pain is a relatively common symptom in children and adolescents. According to some estimates, about 80% of children will have at least one episode of lower back pain by the age of 20 years. The most common type of low back pain in children is non-specific pain in the lower back, which is probably caused by muscle stretching, bad posture (scoliosis, Scheuermann’s disease), spondylolisthesis, or herniation of the intervertebral disc. However, systemic inflammatory diseases (juvenile idiopathic arthritis), tumor processes, infections, fractures, and other less common causes should be considered. During history taking and examination of the child, we may find warning signs that suggest serious illness underlying low back pain. These signs include low back pain in a child younger than 10 years, and especially a child younger than 4 years, the presence of systemic signs (fever, fatigue, inappetence, weight loss, diarrhea), local sensitivity in the spinal region, pain at rest or at night, presence of neurological symptoms, including radiculopathy, loss of sensation, muscle weakness, incontinence of urine and stool, presence of morning stiffness, information on recent trauma or infection, current immunosuppressive therapy, and known malignant disease. Children with one or more of these signs should be investigated further or hospitalized. Psychosocial circumstances in the family and school should be checked. In all children, a clinical examination including the bending test, Lasegue’s test, Patrick’s test, and Trendelenburg’s test should be performed. If the symptoms worsen or persist for longer than 4-6 weeks, further workup is required.
References:
1. Naveed A, Heinz P. Joint pain in children. J Paediatr Child Health. 2013;24:45-50.
2. Kordi R, Rostami M. Low back pain in children and adolescents: an algorithmic clinical approach. Iran J Pediatr. 2011;21:259-70.
3. Versus Arthritis. Musculoskeletal clinical assessment in children and young people: pGALS questions and examination [Internet]. Versus Arthritis; [cited 2025 Mar 6]. Available from: https://versusarthritis.org.
4. Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM. Nelson Textbook of Pediatrics. 21st ed. Philadelphia, PA: Elsevier; 2020. Chapter on Pediatric Rheumatology and Joint Disorders.
5. Jelušić M, Malčić I, editors. Pedijatrijska reumatologija, 1st ed. Zagreb: Medicinska naklada, 2014.
More posts for medical professionals




